What is amenorrhea?
Amenorrhea refers to the absence of menstrual periods. It is classified into two main types:
- Primary amenorrhea: When menstruation has not started by age 15 in girls with otherwise normal growth and secondary sexual characteristics, or by age 13 if there are no signs of puberty.
- Secondary amenorrhea: When a woman who previously had regular cycles stops having periods for three or more months (six months if her cycles were previously irregular).
While missing one or two periods is not uncommon, persistent absence of menstruation deserves medical evaluation.
How does the menstrual cycle work?
To understand amenorrhea, it helps to review how a normal menstrual cycle works. Each month, a complex interaction between the hypothalamus, pituitary gland, and ovaries regulates hormones such as FSH (follicle-stimulating hormone), LH (luteinizing hormone), estrogen, and progesterone. These hormones control the maturation of eggs, ovulation, and the thickening/shedding of the uterine lining.
If any part of this hormonal system is disrupted, ovulation and menstruation may not occur.
What are the different causes of amenorrhea?
Amenorrhea can result from a wide range of physiological, structural, and hormonal factors.
1. Physiological Causes
- Pregnancy: the most common and natural cause of amenorrhea
- Lactation: breastfeeding suppresses ovulation through high prolactin levels
- Menopause: permanent cessation of ovarian function, typically at age 51
2. Hypothalamic or Pituitary Causes
- Hypothalamic amenorrhea: disruption in the hormonal center of the brain often due to stress, weight loss, excessive exercise, or eating disorders
- Pituitary tumors: typically benign but suppresses hormone signals to the ovaries
- Thyroid disorders: both hypothyroidism and hyperthyroidism can disrupt menstrual cycles
3. Ovarian Causes
- Premature ovarian insufficiency: depletion of ovarian follicles before age 40
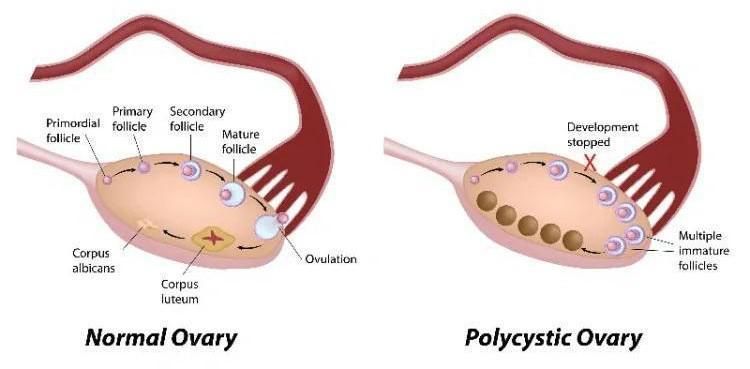
- Polycystic ovary syndrome (PCOS): characterized by irregular ovulation, androgen excess, and polycystic ovaries
- Genetic or chromosomal abnormalities: Turner syndrome (45,XO), Fragile X premutation carriers
4. Uterine and Outflow Tract Causes
- Asherman’s syndrome: scarring inside the uterus, often from prior surgeries or infections
- Congenital anomalies: absence or malformation of the uterus, cervix, or vagina (Müllerian agenesis)
5. Medications and Systemic Illnesses
- Medications: hormonal contraceptives, antipsychotics, or chemotherapy agents
- Chronic illnesses: diabetes or celiac disease
How is amenorrhea diagnosed?
Evaluation begins with a comprehensive medical history and physical examination, followed by targeted laboratory and imaging studies.
Step 1: Exclude Pregnancy
- A urine or serum β-hCG test should always be the first step.
Step 2: Hormonal Evaluation
- FSH and LH: elevated levels suggest ovarian failure; low levels indicate hypothalamic or pituitary dysfunction
- Prolactin: elevated in prolactin-secreting tumors or medication effects.
- TSH: evaluates for thyroid dysfunction
- Estradiol: assesses estrogen status and ovarian function
- Androgens: elevated levels can indicate PCOS or adrenal disorders
Step 3: Imaging
- Pelvic ultrasound: evaluates uterus and ovaries for structural abnormalities or polycystic morphology
- MRI of the pituitary: ordered if prolactin is elevated or pituitary disease is suspected
Step 4: Additional Tests
- Progestin challenge test: determines if estrogen is present and if outflow tract is patent
- Karyotype testing: used in primary amenorrhea to detect chromosomal abnormalities
How is amenorrhea treated?
Treatment depends on the underlying cause and the patient's reproductive goals.
- Lifestyle and Functional Causes
- Nutritional rehabilitation: increase caloric intake and restore healthy body weight
- Stress management: mindfulness, therapy, or reduced physical strain
- Exercise moderation: adjust intensity and duration to restore hormonal balance
- Hormonal Disorders
- PCOS: managed with hormonal contraceptives to regulate cycles, or ovulation induction if fertility desired
- Hyperprolactinemia: treated with dopamine agonists such as cabergoline or bromocriptine
- Thyroid disorders: treated by correcting thyroid hormone levels
- Ovarian Insufficiency
- Hormone replacement therapy (HRT): helps protect bone density and relieve symptoms related to estrogen deficiency
- Structural Causes
- Surgical correction: In cases such as Asherman’s syndrome, hysteroscopic removal of adhesions can restore menstruation
- Congenital anomalies: May require reconstructive surgery or counseling regarding reproductive options
What are the potential complications of untreated amenorrhea?
Chronic absence of menstruation can have long-term health consequences including:
- infertility due to anovulation
- osteoporosis if prolonged hypoestrogenism
- cardiovascular risks associated with hormonal imbalance
- endometrial hyperplasia if unopposed estrogen is present without regular shedding
My period has stopped. Should I see my doctor?
You should seek medical evaluation if:
- you have not started menstruating by age 15
- your periods stop for more than 3 months (and you’re not pregnant)
- you experience symptoms such as hot flashes, hair loss, nipple discharge, or headaches
- you have a history of significant weight changes, stress, or excessive exercise
Key Takeaways
Amenorrhea is not a disease itself but a symptom of an underlying condition. While it is sometimes a normal physiological occurrence (such as during pregnancy or menopause) amenorrhea can also signal underlying medical or hormonal issues that need evaluation. Identifying the cause requires careful evaluation of hormonal, structural, and lifestyle factors. The good news is that many causes are treatable, and menstrual cycles can often be restored with appropriate care. For women who are not menstruating, timely medical attention can safeguard reproductive health, bone strength, and overall well-being.
Get In Touch